Infections
Jump To
Introductions of Eye Infections
Eye infections are a concerning issue that can jeopardize eye health and cause discomfort. Characterized by their diverse nature and impact, all eye infections should be diagnosed and treated. Our specialized team at Idaho Eyelid and Facial Plastic Surgery expertly handles these infections as we focus on preserving your vision and enhancing your ocular well-being. Accurate diagnosis is crucial for effective treatment. Through experience and ophthalmic testings, our skilled specialists determine the specific nature of the infection, enabling us to formulate targeted treatment plans tailored to your individual needs. Moreover, we have expertise to know when infections are easily treatable with home remedies and when conditions dictate more extensive treatment. Do not ignore eye infections as they can lead to more severe complications. Discover how our dedicated expertise ensures your best eye health. It’s our top priority.
Common Eye Infections
Eye infections encompass a spectrum of conditions, each presenting distinct challenges and requiring specific attention. Understanding these varied infections is vital for timely recognition and appropriate management:
- Allergic Conjunctivitis: this condition, often triggered by allergens, leads to inflammation of the conjunctiva, resulting in itching, redness, and excessive tearing.
- Conjunctivitis (Pink Eye): an inflammation of the conjunctiva, commonly caused by viruses, bacteria, or allergies, resulting in redness, irritation, and discharge. Highly contagious.
- Cellulitis: an infection affecting the tissues around the eye, causing redness, swelling, and tenderness, often due to bacterial invasion. This can lead to permanent vision loss and life-threatening complications if left untreated.
- Blepharitis: common and sometimes recurring condition that causes inflammation of the eyelids.
- Corneal Infections: infections that affect the cornea, typically caused by bacteria, viruses, fungi, or parasites, leading to pain, blurred vision, and sensitivity to light.
- Herpes Zoster (Shingles): a viral infection caused by the reactivation of the varicella-zoster virus, presenting with a painful rash and blisters around the eye.
- Lacrimal System Infections: Infections affecting the tear drainage system, causing tearing, discharge, and discomfort due to blockages or inflammation.
- Molluscum Contagiosum: a viral skin infection that can affect the skin around the eyes, causing small, painless bumps. Can spread rapidly especially with eye rubbing.
- Orbital Infections: infections affecting the eye socket, often leading to swelling, pain, and impaired eye movement due to bacterial or fungal invasion.
A note about viral versus bacterial infections… a virus consists of a core of nucleic acid (DNA or RNA) surrounded by a coat of antigenic protein. The virus provides the genetic code for replication, whereas the host cell provides the energy and raw material for the virus to grow. This is different than bacteria, which are single cell organisms that do not have a nucleus and are among the most simple and most abundant life forms on earth. Antibiotics are effective against bacterial infections, not viruses. Bacteria grow outside the host cell and can be attacked by antibiotics.
Allergic Conjuctivitis
Allergic conjunctivitis is the irritation of the conjunctiva, or covering of the eyeball, as a reaction to an allergic substance. Allergic conjunctivitis, which is not contagious, causes one’s eyes to become watery, red, swollen, itchy, and often painful. This condition, which is may also be called allergy eyes, may be acute or chronic, seasonal and perennial. Seasonal allergic conjunctivitis affects people during specific seasons of the year while perennial allergic conjunctivitis impacts people throughout the year. Allergic conjunctivitis can cause much discomfort due to the symptoms listed above. Untreated allergic conjunctivitis can result in eye rubbing, which could lead to permanent eye damage.
A person develops allergic conjunctivitis when exposed to an allergic or sensitive substance, which is referred to as an allergen. Many of these allergens are listed below:
- Pollen. Trees, grass, weeds, and flowers release the allergen pollen into the air. During the spring and fall months, pollen levels are at their highest. Pollen affects those with allergic conjunctivitis by entering the throats and noses of those who are sensitive to the substance. Pollen levels are at the highest during the spring and fall months. Pollen is considered one of the most difficult causes of allergic conjunctivitis to control. Some common types of pollen include ragweed, cedar and ash.
- Mold. Allergen mold is also released through the air, from spores in leaves, grass, and hay. Mold usually impacts those who are susceptible between spring and late fall. Cold temperatures and snow diminish mold spores counts, yet they are still present after frost begins. Mold can also develop in damp atmospheres within the home, such as the kitchen or bathroom.
- Pets. A dog or cat’s dander, or skin flakes, as well as its saliva and urine can be powerful allergens. Although the hair of a pet is not considered a powerful allergen itself, the pet’s hair or fur can collect mold, pollen, and dust.
- Dust mites. Tiny bugs that are related to spiders and ticks also cause allergic conjunctivitis. Cleanliness and moisture levels have impact on the amount of dust mites that may be found in your home. Dust mites can be found on sofas, curtains, bed sheets, and almost anywhere else in the home. By commonly vacuuming and washing bed sheets one can reduce the number of dust mites.
- Pollution. Pollution is commonly associated with allergic conjunctivitis. While it comes in various forms, air pollution, such as the type released from automobiles and factories, is a powerful type of contamination linked to allergic conjunctivitis.
- Other. Some chemicals found in certain cosmetics, carpeting, and paint along with cigarette smoke are also thought to be allergens.

Annoyed by Allergens
Allergens are triggers or instigators of allergic reactions. For those who suffer from allergy eyes, it is helpful to identify the causes of allergic conjunctivitis. A person has a considerably better chance of controlling the condition and avoiding its unpleasant side effects once he or she is aware of the causes. Since allergy eyes can be caused several allergens, some people might want to avoid more than one specific allergen in order to minimize reaction. Although there are a large number of allergens, there are certain types that occur more prevalently with condition than others.
Conjunctivitis (Pink Eye)
Almost all of us have been afflicted by the high contagious Pink Eye, also known as conjunctivitis. It is an infection of the conjunctiva (the inside of the eyelid) and can be caused by bacteria, virus or allergies (covered in the Allergic Conjunctivitis section). Typical signs of Pink Eye include red, irritated, watery eyes with a burning and scratchy feeling. Many people also have pus or a watery discharge. Treatment usually involves an antibiotic selected by your eye care specialist. To prevent the spread of infection, wash hands before and after using medicine in your eye. Wash any clothes, towels, pillow cases touched by the infected eye. Avoid sharing cosmetics.
Blepharitis
Blepharitis is a common and sometimes recurring condition that causes inflammation of the eyelids. It usually affects both eyes along the edges of the eyelids and typically occurs when the oil glands near the base of the eyelashes become clogged, often causing redness/irritation. Several diseases and conditions can cause blepharitis. It can be difficult to treat, and although uncomfortable and unsightly, does not usually cause permanent damage to your eyesight and is not contagious. Chalazion, a painless firm lump caused by inflammation of the oil glands of the eyelid, is a condition that is sometimes associated with blepharitis.
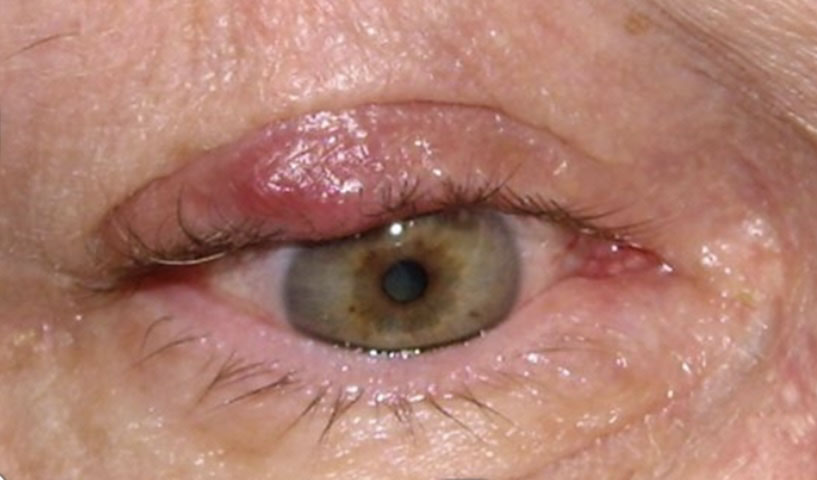
Patient with Chalazion
Blepharitis occurs in two forms, anterior blepharitis and posterior blepharitis. Anterior blepharitis affects the outside front of the eyelid, where the eyelashes are attached. The two most common causes of anterior blepharitis include bacteria (staphylococcus) and scalp dandruff. Posterior blepharitis also impacts the inner eyelid (the moist part that makes contact with the eye) and is caused by problems with the oil glands in this part of the eyelid. Two skin disorders can cause this form of blepharitis, including acne rosacea, which leads to red and inflamed skin, and scalp dandruff. Symptoms and treatment are briefly presented below:
- Symptoms associated with blepharitis include: dry eye, foreign body, burning sensation, excessive tearing, itching, sensitivity to light (photophobia), red and swollen eyelids, redness of the eye, crusting of the eyelashes on awakening
- Treatment involves helping patients keep the eyelids clean and free of crusts. Warm compresses can loosen the crusts, followed by a light scrubbing of the eyelid with a cotton swab and a mixture of water and baby shampoo. Patients who have acne rosacea should have that condition treated at the same time.
Bacterial Keratitis (Corneal Ulcer)
A corneal ulcer is an infection of the cornea by bacteria, viruses or fungi. Two of the common causes are abrasion of the cornea with foreign bodies and poor hygiene of contact lenses (especially if worn overnight). Signs of a corneal ulcer include eye pain, redness, itching and burning, white patch on the cornea, increased tearing, sensitivity to light (photophobia).

Example of a Corneal Ulcer
Early attention by an ophthalmologist or optometrist to any eye infection might prevent the ulceration and further injury to the cornea. An untreated corneal ulcer can permanently damage the cornea. It might also perforate the eye, resulting in a spread of infection and increasing the risk of permanent visual impairment.
Herpes Zoster (Shingles)
Herpes zoster is caused by the herpes simplex virus. It is the same virus which causes cold sores and genital herpes. Infection can be spread to the eye by touching an active lesion and then the eye. Such infections of the eye can lead to pain, swelling, redness, light sensitivity, and even blurred vision. It specifically affects the cornea of the eye through ulceration (keratitis). Repeated episodes of herpes zoster infection are associated with other eye conditions, including glaucoma, scarring inside the eye, and cataract formation.

Example of Herpes Zoster
Lacrimal (Tear System)
There are a number of lacrimal infections that we see commonly at Idaho Eyelid and Facial Plastic Surgery: Dacryoadenitis, Canaliculitis, Dacryocystitis, Acute Dacryocystitis and Chronic Dacryocystitis. Each of these infections is briefly described below:
- Dacryoadenitis is inflammation of the tear-producing lacrimal gland. This condition may occur with systemic diseases such as Sjogren’s, sarcoidosis, syphilis, TB, lymphoma, and benign lymphoid hyperplasia and may occur in patients with mums, EBV, zoster. Symptoms include pain, tenderness, and swelling of the lateral aspect of the eyelid. Complications from dacryoadenitis are rare, although a lacrimal gland abscess may develop. The infection may lead to preseptal or orbital cellulitis as well. It is typically treated with systemic broad spectrum antibiotics and abscess drainage when necessary.
- Canaliculitis is another infection. Each eye has two canaliculi, one for the upper eyelid and one for the lower. The canaliculus (plural, canaliculi) is a short channel near the inner corner of the eyelid through which tears drain into the tear sac. Canaliculitis is an inflammation, usually caused by infection of the canaliculus. Symptoms include pain, swelling, tenderness of the inner canthus of the eye. It may be treated with Penicillin irrigation. Typically this infection impacts those individuals over 40 years of age. It can turn into a chronic inflammation of the canalicular system and can remain undiagnosed for a long period of time because it is rare and has a variable presentation.
- Dacryocystitis is an infection of the nasolacrimal sac and sometimes coincides with a blockage of the nasolacrimal duct. It can be acute or chronic and congenital or acquired. Medial canthal swelling of dacryocystitis is usually located below the medial canthal tendon. Symptoms include acute onset, tearing from nasolacrimal duct obstruction, redness, discharge, and tender and swollen lacrimal sac. If the tearing causes severe symptoms, surgery can be performed to create a new tear duct. Silicone tubes are placed in the tear system to keep the new tear duct open while healing occurs.
- Acute dacryocystitis is characterized by a nasolacrimal duct obstruction impacting drainage from the lacrimal sac to the nose. It can involve chronic tear stasis causing a secondary infection, edema, and erythema below medial canthal tendon with lacrimal sac distention. Warm compresses may help, along with oral/IV antibiotics such as Keflex, Augmentin (topical antibiotics have limited value). Complications include mucocele, chronic conjunctivitis, and/or orbital cellulitis. Most patients require a DCR after acute infection subsides.
- Chronic dacryocystitis is characterized by a distended lacrimal sac with minimal inflammation and suppurative discharge from the punctum. It is important to probe/irrigate upper system only. Again, patients usually need DCR for resolution.
Molluscum Contagiosum
Molluscum contagiosum is a viral infection that is exclusive to humans. It is characterized with the presence of small elevated lesions called papules. These papules have a waxy surface and are seen on various parts the body such as the face, trunk, arms and legs. It can also affect the armpits but does not involve the palms. It has also been found to affect the eyelids. Molluscum contagiosum is caused by a viral infection. The portal of entry of the riders into the body is usually through some form of break in the skin. Having low levels of immunity such as in the case of HIV virus infections can also make an individual prone to developing molluscum contagiosum. In such individuals, the lesions are a lot more widespread. Studies have also shown the development of molluscum contagiosum affecting the eyelids of both eyes following treatment of rheumatoid arthritis with specialist drugs such as methotrexate.
Molluscum contagiosum is caused by a DNA poxvirus called the molluscum contagiosum virus (MCV). MCV has no animal reservoir, infecting only humans. There are four types of MCV, MCV-1 to -4; MCV-1 is the most prevalent and MCV-2 is seen usually in adults and often sexually transmitted. This common viral disease has a higher incidence in children, sexually active adults, and those who are immunodeficient. The infection is most common in children aged one to ten years old. The virus commonly spreads through skin-to-skin contact. This includes sexual contact or touching or scratching the bumps and then touching the skin. Handling objects that have the virus on them (fomites), such as a towel, can also lead to in infection. The virus can spread from one part of the body to another or to other people. The virus can be spread among children at day care or at school. Molluscum contagiosum is contagious until the bumps are gone; which, if untreated, could be up to 6 months or longer. The time from infection to the appearance of lesions can range up to 6 months, with an average incubation period between 2 and 7 weeks.

Example of a Patient with molluscum contagiosum
Multiple small papules with a waxy/shiny surface become clearly evident on the body, and are particularly noticeable on the eyelids. Typically, scratching the lesions can make them worse as more and more lesions form along the line of scratching. This is a typical phenomenon called as Koebner phenomenon. Upon examination, the lesions are flesh colored and vary between 2 to 5 mm in size. Patients with poor immune levels tend to have multiple lesions all over the body. The involvement of the eyelids and the face is commonly seen in children whereas the involvement of the groin area is seen in adults. Associated with molluscum contagiosum are other skin conditions such as atopic dermatitis and eczema. Regarding diagnosis and treatment of molluscum contagiosum:
- Diagnosis. A polymerase chain reaction test and/or excisional biopsy can be ordered. A biopsy demonstrates the presence of specific structures within the lesions called inclusion bodies. These bodies can be stained using specific dyes to help identify them under a microscope. Diagnosis is also made on the clinical appearance. Molluscum contagiosum lesions are flesh-colored, dome-shaped, and pearly in appearance. They are often 1–5 millimeters in diameter, with a dimpled center. They are generally not painful, but they could itch or become irritated. Picking or scratching the bumps could lead to further infection or scarring. In about 10% of the cases, eczema develops around the lesions. They could occasionally be complicated by secondary bacterial infections. In some cases the dimpled section could bleed once or twice. The viral infection is limited to a localized area on the topmost layer of the epidermis. In a process called auto-inoculation, the virus can spread to neighboring skin areas. Children are particularly susceptible to auto-inoculation, and could have widespread clusters of lesions.
- Treatment. Once the virus containing head of the lesion has been destroyed, the infection is gone. The central waxy core contains the virus. One form of treatment is called curettage and involves administration of an anaesthetic agent followed by removal of the lesion completely. Most cases of molluscum contagiosum tend to resolve themselves in a few months. Depending on the severity of the case, it is possible that molluscum contagiosum impacting eyelids could be managed conservatively without performing any intervention. Although other treatments are available to manage molluscum contagiosum, detailed studies have shown that there does not appear to be any additional benefit of using these treatments (skin creams, anti-viral agents and herbal medicines) in comparison to doing nothing at all.
Orbital Infections
Orbital infections affecting the eye socket often lead to swelling, pain, and impaired eye movement due to bacterial or fungal invasion. An orbital abscess is a collection of pus within the eye socket, usually secondary to a severe orbital infection, causing pain, fever, and visual disturbances.They can be vision- and life-threatening, and prompt evaluation and treatment of patients with these infections is essential. At Idaho Eyelid and Facial Plastic Surgery, our medical team can facilitate an accurate diagnosis and treatment plan in Boise, Idaho. Orbital and preseptal cellulitis both present risks:
- Orbital cellulitis is usually a complication of paranasal sinus infection, is an infectious inflammatory process involving the orbital tissues posterior to the orbital septum, and may necessitate orbital fracture repair and strabismus surgery. Extension of pre-existing infections of the face, lacrimal sac, and lacrimal gland can extend into the orbit and present complications. Prompt treatment is mandatory to avoid visual loss or intracranial complications. Initially, IV antibiotics might possibly be administered, but if no improvement appears within 48h, surgical drainage of the orbit and the affected sinuses must be performed. Without appropriate treatment orbital infection might possibly lead to serious complications, even death.
- Preseptal cellulitis (periorbital cellulitis) is an infectious inflammation of the tissues anterior to the orbital septum, and is more often experienced in children with upper respiratory infections. The most common bacterial pathogens in preseptal cellulitis include Haemophilus influenza, Staphylococcus aureus, and Streptococcus pneumonia. It is possible for teens/adults to be closely followed as outpatients with oral antibiotics but if their condition worsens then a CT scan and/or IV antibiotics may be needed. Patients under 5 years old might possibly have bacteremia, and may require stronger antibiotics after blood cultures are taken. Infants with preseptal cellulitis are usually admitted for intravenous therapy. Surgical drainage of abscesses may be required. Subperiosteal abscess formation should be suspected if patients fail to improve or deteriorate on intravenous antibiotics.
At Idaho Eyelid and Facial Plastic Surgery, we prioritize understanding and addressing these infections promptly to ensure effective eye infection treatments and prevention. Whether it’s conjunctivitis, bacterial or viral infections, our clinic provides tailored solutions to manage and resolve these concerns for our Boise community and beyond. Our clinic offers a spectrum of treatment options depending on the diagnosis, from antibiotic eye drops to innovative therapies. We believe in a comprehensive approach that includes both conventional medical treatments and complementary measures, including safe home remedies, ensuring optimal recovery and comfort. We boast an experienced team of seasoned ophthalmologists and eye infection experts dedicated to providing exceptional care. With our commitment to precision, experience, and patient-centric approaches, we assure you of comprehensive care tailored to your needs. At Idaho Eyelid and Facial Plastic Surgery, your ocular health is our priority. Allow us to be your partner in preserving and enhancing your vision. Book your consultation today with our eye specialist in Idaho and experience the expertise and compassionate care we offer.

